New to Mental Health Real Talk?
Create an account to get started today.

As much as I would love to be one of those people who jumps out of bed in the mornings, wide eyed, refreshed and ready to take on the day ahead, it just isn’t me. I am not a morning person at all. That being said, on the good days when I plan things to look forward to, or am in a good head space, mornings are inevitably easier. However, on the difficult mornings, my bed holds me hostage. I don’t want to face the day, I don’t want to wake up and I certainly don’t want to leave the cosy sanctuary of my blankets.
But I have found something that helps. I call it the “one hour rule.”
Within one hour of waking up, I have to be out of my bed. If I look at the clock when I wake up and it is 9 a.m., by 10 a.m., I cannot still be lying in bed. I am a competitive person, and even some gentle competition with my own brain helps me sometimes.
I tell myself: Just try. Get out of bed and get up. If it doesn’t work, and in an hour you feel worse, then you can go back to bed. And sometimes, I will. And that’s OK. But I make myself try. Try to taste the day. I don’t have to like it, I just have to do it.
I have to be up though. I have to be doing or moving or creating. It can work like a domino effect. If I am up, I may as well take a shower,
may as well make some breakfast, and hey — seeing as I’m already up, I might just leave the house today.
I can’t promise that it always works like this, but one thing I do know is that I always feel better for giving it a go.
I encourage you to give yourself one hour, 60 minutes, 3,600 seconds.
It might suck, and you may get out of your bed just to end up on the floor instead, or sitting on the landing, or you might make it to sit on the shower floor. But at least you tried. You got up and you gave today a chance. You did the absolute best that you could, and there is no shame in that. It does not go unnoticed.


The teenage years are often characterized by peer pressure, styles you never thought would come back in fashion and of course — angst. But what we may fail to recognize is that many teens are really hurting. For some, the teenage years are a time marked by emotional abuse.
The adults who experienced emotional abuse as teenagers may have been the teens who were struggling academically, the ones with the tough exteriors or the ones who seemed to have it all “figured out.” The effects of emotional abuse present differently in every individual. It’s important to remember we never know what may be going on in the life of a young person, so we should strive to treat them with compassion and respect.
We wanted to know what kinds of effects emotional abuse in the teenage years can have on adulthood, so we asked our mental health community to share one thing they do now that stemmed from the emotional abuse they experienced as a teenager.
No matter what your experience of emotional abuse was, it is important to remember hope is never lost and there is help out there.
Here’s what they had to say:
1. “If anything goes wrong, I immediately determine how it was my fault, and rehearse my explanation/apology. I then commence calling myself names and criticizing myself for allowing it to happen.”
The teenage years are often characterized by peer pressure, styles you never thought would come back in fashion and of course — angst. But what we may fail to recognize is that many teens are really hurting. For some, the teenage years are a time marked by emotional abuse.
The adults who experienced emotional abuse as teenagers may have been the teens who were struggling academically, the ones with the tough exteriors or the ones who seemed to have it all “figured out.”

Movies have always made me feel less alone in the world. They make me feel like there is always someone out there who understands. Who has gone through the same things as me. Who fights the same wars I do. Who just gets it.
When I was first diagnosed with bipolar disorder, I watched all the movies about mental illness I could get my hands on. They genuinely helped me. They gave me characters I could identify with and situations I related to. They taught me a lot about what it means to live with a mental illness and how to overcome some of the struggles that come with having a disorder. They also taught me how to help someone else who is struggling with a disorder and how I could be there for them. They taught me what to do and what not to do and ultimately gave me hope for the future.
Movies have always made me feel less alone in the world. They make me feel like there is always someone out there who understands. Who has gone through the same things as me. Who fights the same wars I do. Who just gets it.
When I was first diagnosed with bipolar disorder, I watched all the movies about mental illness I could get my hands on. They genuinely helped me. They gave me characters I could identify with and situations I related to. They taught me a lot about what it means to live with a mental illness and how to overcome some of the struggles that come with having a disorder. They also taught me how to help someone else who is struggling with a disorder and how I could be there for them. They taught me what to do and what not to do and ultimately gave me hope for the future.
So here are 10 movies about mental illness that have helped me in one way or another along the way. Not all of them have happy endings, but there is still something to learn from each of them. Most are about bipolar disorder because that’s what I can relate to, but there are some other disorders mentioned too. Warning — some movies may be triggering.


I’m scared my mental illness makes me unlovable. It’s a statement I hate writing and a sentence I hate thinking about. But it’s how I feel. I feel like as my depression and anxiety become more chronic issues, my thoughts about falling in love and the chances of it happening to me start to slim. While this is a small part of me, I can’t help but feel as though there is a giant neon sign following me.
The truth is, when I tell the people I’m dating it usually starts out OK. They seem to understand and accept this is a part of me, but it isn’t all me. But the further we get down the path of being together and the more they realize how much it actually affects my everyday life, that is when I see them start to look for the exit.
I’ve had exes tell me they can’t make me feel better because I’m letting these “issues” consume me. I’ve had exes tell me they don’t feel as though they can tell me the truth about things because they’re worried it’ll send me into a tailspin. I’ve had exes try to tell me how to manage my illnesses even though they’ve never experienced it themselves.
I don’t need someone to tell me what to do or how to do it when it comes to depression or anxiety. All I want, all I truly want, is someone just to love me through it. That’s the part that is sometimes lost on potential partners. I don’t need someone to fix me. I go to therapy. I take my medication. I work hard each and every day to ensure I am doing all I can to prevent the bad days from occurring more often than not.
What I do need is for someone to just be there when things get hard. When those bad days come on and I can’t think of a reason why I should get out of bed, I want someone to be there to just tell me I can do it. I want someone to hold me when, in the middle of the night, I can’t breathe because my anxiety is out of control. I want to be able to tell someone my deepest darkest secrets when it comes to my illness and not have them look at me like I have three heads.

As a nurse working in the emergency department, I frequently see people come in for suicide attempts. I’ve noticed there’s a stigma surrounding some attempts, and many colleagues agree there’s a difference in the way patients are treated depending on the type of attempt.
From what I’ve seen, a patient whose attempt is more “serious,” with visible life-threatening injuries or potentially deadly pathology results, is more likely to be treated with understanding, compassion and patience. It’s as if serious injuries validate the mental illness, making the inner turmoil visible to the outside world.
But the “less serious” the attempt is (for example, taking a non-lethal amount of medication or self-inflicted injuries that aren’t fatal), the less sympathy I’ve seen patients receive. This can also be said for patients who have repeat suicide attempts. I’ve heard these patients referred to as “time-wasters,” “attention-seekers,” “taking up beds,” and they’re described as “crying out for help.” Although it’s acknowledged as wrong, there’s still anger and frustration felt towards the patient. I’ve heard many question the reason for their behavior. But I believe anyone who intentionally puts themselves in harm’s way needs help, regardless of the intended outcome, and are still entitled to be treated with dignity, understanding and kindness.
When I was 23, I tried to jump off a cliff after being discharged from a psychiatric hospital. I have bipolar affective disorder. I rarely call this a suicide attempt, although I would’ve jumped if it weren’t for a person walking past.
Graduate from high school. Go to college. Get a job.
That’s how it’s “supposed” to go.
But, life happens. Mental illness happens. And not everyone ends up in school, or in the workforce. Or some people enter the workforce, and then have to leave.
We’re here to tell you, that’s OK.
Whether you’re not working because managing your mental health is a full-time job, a “typical” work environment just doesn’t work with your brain or if you just need a break to focus on getting well, just because you’re not working, doesn’t mean you’re useless.
It can be hard to believe this when people assume you’re not working because you’re lazy, or pass judgment your way. So we wanted to know what people who are currently unemployed and living with a mental illness wish others understood. Because no matter what’s stopping you from working right now, you’re definitley not alone.
Here’s what our community told us:
1. “Just because I can’t hold a job doesn’t mean I’m lazy or a bad person.”
Graduate from high school. Go to college. Get a job.
That’s how it’s “supposed” to go.
But, life happens. Mental illness happens. And not everyone ends up in school, or in the workforce. Or some people enter the workforce, and then have to leave.
We’re here to tell you, that’s OK.
Whether you’re not working because managing your mental health is a full-time job, a “typical” work environment just doesn’t work with your brain or if you just need a break to focus on getting well, just because you’re not working, doesn’t mean you’re useless.
It can be hard to believe this when people assume you’re not working because you’re lazy, or pass judgment your way.

On Thursday, John Green announced his new book, “Turtles All the Way Down,” which comes out later this year, is inspired by his own experiences with mental illness, namely obsessive-compulsive disorder (OCD). Green is best known for his book “The Fault in Our Stars,” which was turned into a movie in 2014.
Green said in a statement that he has been working on “Turtles All the Way Down” for years and that “this is my first attempt to write directly about the kind of mental illness that has affected my life since childhood, so while the story is fictional, it is also quite personal.”
Green has been open about his experiences with anxiety and OCD in the past and has been an advocate for the destigmatization of mental illness.


1. What they are and why I’ve been prescribed them. It’s surprising and pretty scary the number of doctors who will flippantly say, “Do you want to try X?” or “I’m putting you on Y,” without telling you what it is or does. In the hospital I’ve been written up for medications without being told I have been, as an outpatient I’ve had doctors think out loud about various drugs that might help without telling me anything about them, and on more than one occasion I’ve gone home, googled my new prescription and have been left puzzled as to why I was put on an antipsychotic or beta blocker for anxiety because no one told me that off-labelling was a thing…
2. Off-labelling is a thing! Basically, drugs do more than they say on the tin, and can be beneficial for other illnesses, as well as the ones they were designed to treat. Quetiapine (an antipsychotic) can be used as a mood stabilizer, Olanzapine (an antipsychotic) can be helpful for anorexia, lithium (a mood stabiliser) can be used in treatment resistant depression, Amitriptyline (an antidepressant) can help with pain, and Propranolol (a beta blocker) can actually help ease symptoms of anxiety. Who knew? So don’t be alarmed or put off by strange names or descriptions on your pill packet — and ask your psychiatrist if you’re not sure why you’ve been prescribed a specific medication.
3. Side effects. Before I was put on lithium, side effects of various mood stabilizers were explained by one psychiatrist, but that was the first time in six years of being on psychiatric drugs that side effects were ever mentioned. I get that sometimes being aware of side effects beforehand can put people off taking certain medications.

The hallmarks of Narcissistic Personality Disorder (NPD) are grandiosity, a lack of empathy for other people, and a need for admiration. People with this condition are frequently described as arrogant, self-centered, manipulative, and demanding. They may also concentrate on grandiose fantasies (e.g. their own success, beauty, brilliance) and may be convinced that they deserve special treatment. These characteristics typically begin in early adulthood and must be consistently evident in multiple contexts, such as at work and in relationships.
People with narcissistic personality disorder believe they are superior or special, and often try to associate with other people they believe are unique or gifted in some way. This association enhances their self-esteem, which is typically quite fragile underneath the surface. Individuals with NPD seek excessive admiration and attention in order to know that others think highly of them. Individuals with narcissistic personality disorder have difficulty tolerating criticism or defeat, and may be left feeling humiliated or empty when they experience an injury in the form of criticism or rejection.

The American Psychological Association (APA) defines anxiety as an emotion characterized by feelings of tension, worried thoughts and physical changes like increased blood pressure.
It is important to know the difference between normal feelings of anxiety and an anxiety disorder that requires medical attention.
The American Psychological Association (APA) defines anxiety as an emotion characterized by feelings of tension, worried thoughts and physical changes like increased blood pressure.
It is important to know the difference between normal feelings of anxiety and an anxiety disorder that requires medical attention.
When faced with potentially harmful or worrying triggers, feelings of anxiety are not only normal but necessary for survival.
Ever since the earliest days of humanity, the approach of predators and incoming danger has set off alarms in the body and allowed an individual to take evasive action. These alarms become noticeable in the form of a raised heartbeat, sweating, and increased sensitivity to surroundings.
A rush of adrenaline in response to danger causes these reactions. This adrenaline boost is known as the ‘fight-or-flight’ response. It prepares humans to physically confront or flee any threats to safety.
Showing 10 out of 20


A Step by Step Guide: How to Cite a Website in MLA 8, Retrieved March 9, 2019, easybib.com/guides/citation-guides/mla-format/how-to-cite-a-website-mla/
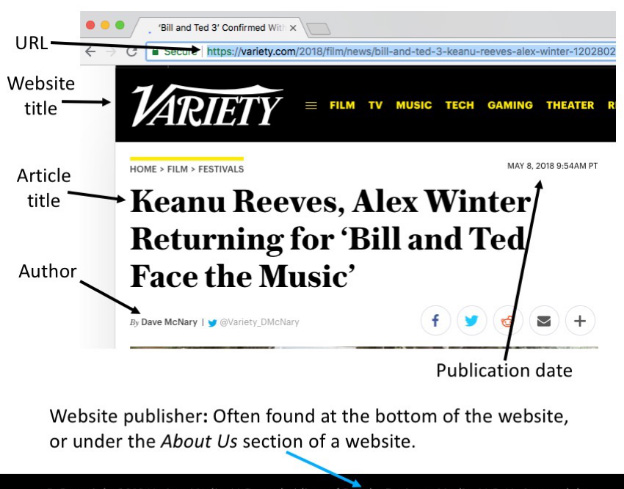
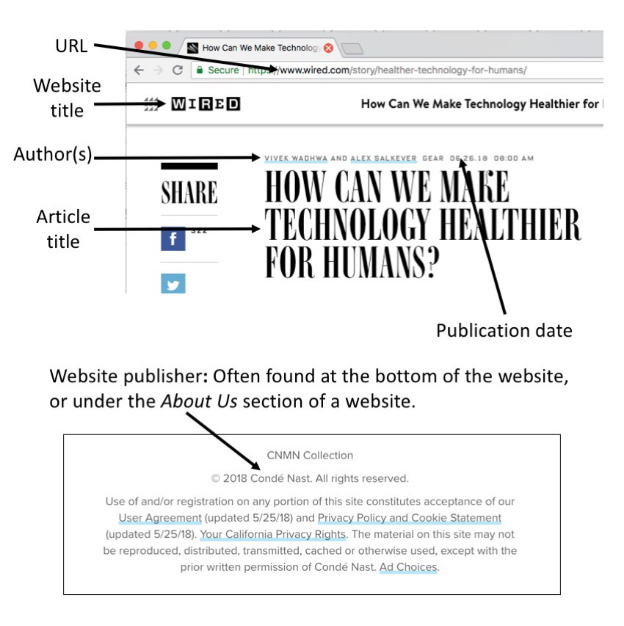
To make an MLA 8 citation for a website, you will need the following pieces of information:
Place the author’s name in reverse order, the last name first, followed by a comma, and then the first name followed by a period. The title of the web page or article is placed in quotation marks, with a period before the end quotation. The title of the website is written in italics followed by a comma. If the name of the publisher differs from the name of the website, include it after the title. Immediately following the publisher is the date that the page or article was published, or posted. Finally, end with the URL, permalink, or DOI.
Sometimes, websites do not state who wrote the information on the page. When no author is listed, you may omit the author information from the MLA citation for the website and begin, instead, with the title.
How to cite a website with no author in MLA 8:

When citing a web page that does not include a formal title, it is acceptable to include a description of the page. Do not place the description in italics or quotation marks. Follow the description with the name of the website.
In an increasingly digital world, social media platforms have become one of the most popular sources students turn to when writing a research paper. When citing social media in your work, follow the same format as an MLA citation for a website. Here are some examples of ways you can cite various social media platforms in your work:
To cite a tweet, you will begin with the account holder’s twitter handle, followed by a period. After this, in quotations, you should enter the full text of the tweet, including any hashtags. The publisher, Twitter, is then listed in italics, followed by the date in Day, Month, Year format and the time the tweet was posted. Finally, include a URL to the tweet followed by a period.

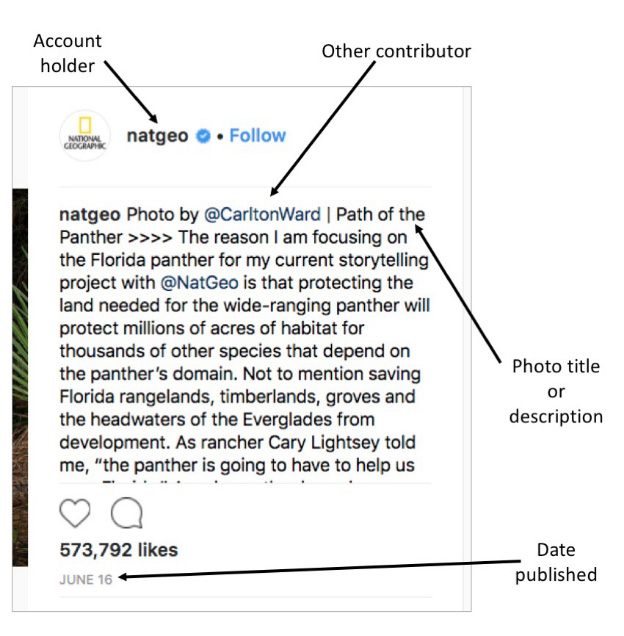
To cite an Instagram post, begin with the account holder’s name or username. In quotations, list the title of the photo, if it is given. If there is no title, write a brief description of the picture but do not place it in italics or quotation marks. The publisher, Instagram, is then listed in italics. Any other contributors (such as the photographer, if it is not the same as the account holder) are then listed, after which you will add the date and URL.
To cite a Facebook post, begin with the account holder’s name or username. In quotations, list the title of the post, if it is given. If there is no title, write a brief description of the post but do not place it in italics or quotation marks. The publisher, Facebook, is then listed in italics, after which you will add the date, time posted, and URL.
Citing the comments left on social media or a website begins with the commenter’s name or username. To indicate that you are citing a comment, follow the name with a period and then the words Comment on, followed by the title of the source (for example, the name of the article) in quotation marks. This is then followed by the title of the website in italics, and the publisher, if applicable. The date and time stamp are then listed, followed by the URL, permalink, or DOI.
How to Cite a Website in APA, March 16, 2019, Retrieved from http://www.easybib.com/reference/guide/apa/website
Structure:
Example:
Structure:
Example:
How to Cite a Website in APA, March 16, 2019, Retrieved from http://www.easybib.com/guides/citation-guides/apa-format/how-to-cite-a-website-apa/
Example:
Structure: